
Something unusual is happening in chronic care management right now. The federal government and the nation's largest private insurer are moving in opposite directions on one of the most consequential questions in healthcare: should technology-enabled chronic care be expanded or restricted?
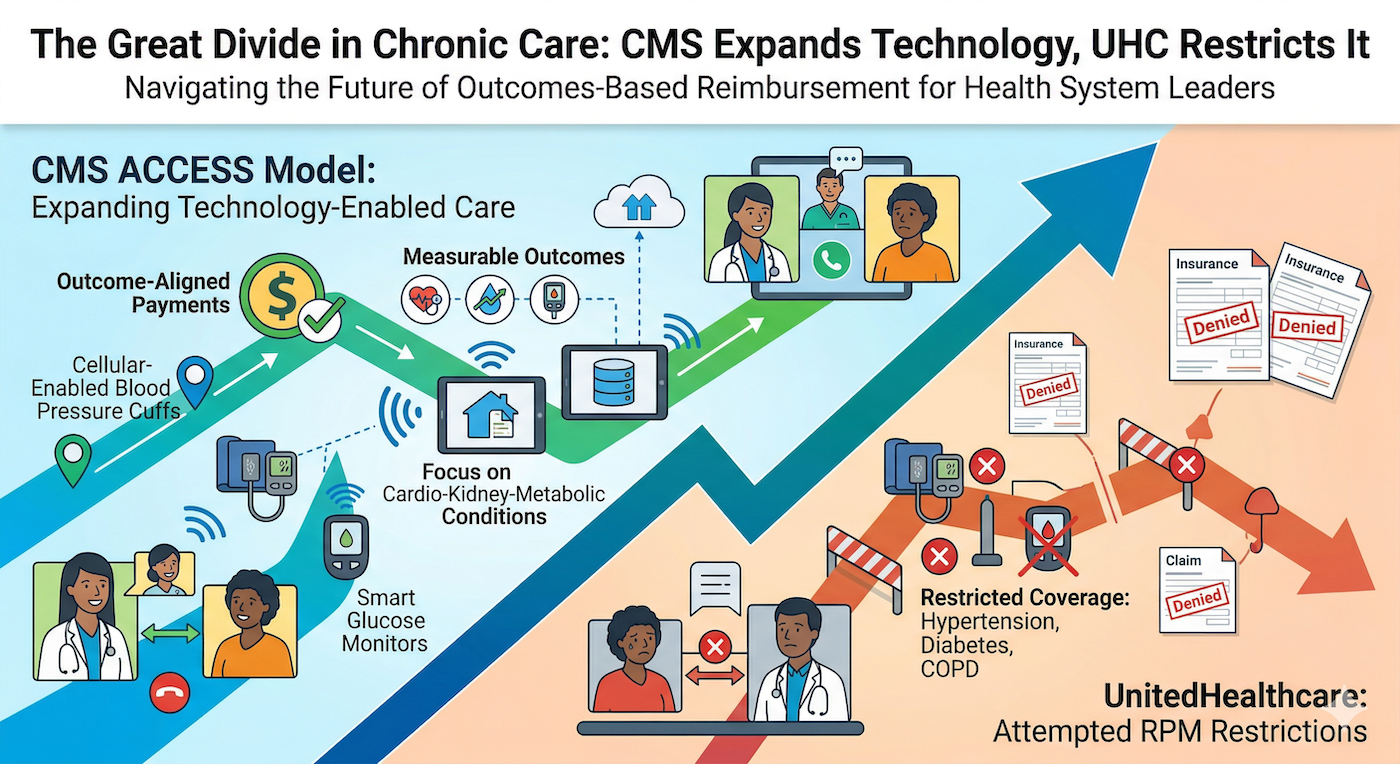
CMS just opened its new ACCESS model for applications, a 10-year initiative launching July 5, 2026, that ties payments directly to measurable patient outcomes. Meanwhile, UnitedHealthcare spent the end of 2025 trying to gut RPM coverage for the conditions that need it most, including chronic hypertension, diabetes, and COPD.
If you are running a health system or provider organization, this divergence is not academic. It will shape your revenue model, your staffing strategy, and your clinical outcomes for the next decade.
ACCESS stands for Advancing Chronic Care with Effective, Scalable Solutions. It is a voluntary CMMI model that tests what CMS calls "Outcome-Aligned Payments," a fundamentally different approach to reimbursing technology-supported chronic care.
Here is how it works. Participating organizations receive recurring payments for managing patients with qualifying chronic conditions. But those payments are not guaranteed. Full payment is tied to achieving measurable health outcomes. In the first model year, the outcome achievement threshold is set at 50 percent, meaning an organization earns its full payment if at least half of its aligned beneficiaries meet the required outcome targets. Fall below that threshold, and payments get reduced proportionally.
The initial clinical focus areas are cardio-kidney-metabolic conditions: diabetes, chronic kidney disease, and atherosclerotic cardiovascular disease. These are not random choices. They represent the costliest chronic disease burden in Medicare, and they are also the conditions where technology-supported interventions have the strongest evidence base.
The model explicitly requires the use of FDA-cleared hardware and software devices. It encompasses clinician consultations, lifestyle and behavioral support, medication management, and care coordination. In other words, it is not paying for a device sitting on a patient's nightstand. It is paying for the clinical program wrapped around that device.
This is the clearest signal CMS has ever sent that technology-enabled chronic care is not a nice-to-have. It is the expected standard of care, and they want to pay for it based on whether it actually works.
Contrast that with what UnitedHealthcare attempted at the start of 2026. The insurer announced that RPM would only be billable for two qualifying conditions: heart failure and gestational hypertension. Patients managing chronic hypertension, diabetes, or COPD would lose RPM coverage entirely across Medicare Advantage, UnitedHealthcare Community Plan, and commercial plan members.
The backlash was swift and intense. RPM advocacy groups, provider organizations, and clinical leaders pushed back hard. UnitedHealthcare ultimately postponed the policy, stating they still intend to implement it in 2026 but have not finalized the timeline.
The logic behind the rollback, that RPM lacks sufficient evidence for these conditions, does not hold up to scrutiny. Health Affairs published a direct rebuttal noting that UHC's position "misreads the evidence and jeopardizes care." The clinical data on RPM for hypertension and diabetes management is extensive. At Welby Health, we see it in our own outcomes every day: patients using cellular-enabled blood pressure cuffs achieve a 20% decrease in blood pressure, and patients using smart glucose monitors see a 20% or greater reduction in blood glucose within four weeks. Our heart failure patients are 5.5 times more likely to adhere to life-saving therapies when enrolled in our programs.
This is not a debate about whether the technology works. It works. The question is whether payers will pay for what works.
If you are a CFO evaluating your chronic care strategy, the CMS ACCESS model represents a meaningful new revenue opportunity, but only if you can actually deliver outcomes. The days of billing for time-based RPM codes without accountability for results are numbered. CMS is telling the market, clearly, that the future is outcome-aligned.
If you are a CMO, the ACCESS model validates what you likely already know: clinical programs that combine licensed clinicians with technology-powered workflows produce better results than either alone. The model requires services that span the full care continuum, from device deployment to medication management to behavioral support. Checking boxes on a time log is not going to cut it.
And if you are a CEO trying to figure out your workforce strategy, consider this: administration comprises 25% of all healthcare costs, and the workforce that handles billing, coding, and patient access is aging out with no reliable pipeline behind them. AI-powered clinical workflows are not replacing nurses and care managers. They are making it possible for a finite clinical workforce to manage larger patient panels while maintaining quality. Our model at Welby pairs licensed RN case managers with AI-powered workflows that automate vital sign monitoring, medication adherence tracking, and patient communication. That combination is what allows us to scale without sacrificing the clinical relationship.
UnitedHealthcare's attempted rollback is a rearguard action. The structural forces driving technology-enabled chronic care forward are too strong.
CMS is not just launching ACCESS. At HIMSS26, CMS Administrator Dr. Oz pushed for agentic AI adoption across Medicare, asking why AI agents could not be introduced for every Medicare beneficiary by the end of the year. More than 700 healthcare organizations have joined the CMS Health Tech Ecosystem pledge. New RPM and APCM CPT codes for 2026 are expanding the eligible patient population and making remote care programs more financially sustainable for the first time in five years.
The momentum is clear. The providers and health systems that build clinical programs capable of delivering measurable outcomes through technology-supported care will be positioned for the next decade. Those waiting for every payer to get on board before investing will find themselves playing catch-up.
The ACCESS model's first performance period begins July 5, 2026. Applications for the January 2027 cohort will follow. If your organization has the clinical infrastructure to manage chronic conditions with technology and the confidence to tie your payments to outcomes, this is the model to watch.
If you do not have that infrastructure yet, the time to build it is now. Not because of one CMS model, but because the entire trajectory of healthcare reimbursement is moving toward paying for what works. The organizations that figure out how to consistently deliver outcomes at scale will win. Everyone else will be negotiating fee schedules on a shrinking pie.
TL;DR: CMS is launching the ACCESS model in July 2026, a 10-year initiative that ties chronic care payments directly to measurable patient outcomes rather than time-based billing. At the same time, UnitedHealthcare tried to gut RPM coverage for chronic hypertension, diabetes, and COPD, only to postpone after industry backlash. These opposing moves create a defining moment for health system leaders. The future of chronic care reimbursement is outcome-aligned, and organizations that can deliver measurable results through technology-supported clinical programs will capture the opportunity. Those waiting for universal payer alignment before investing will fall behind.