Most medical groups say they're "doing CCM." The numbers say they're barely scratching the surface.
There's a conversation I keep having with medical group leaders that goes almost exactly the same way every time.
"We're already doing CCM internally."
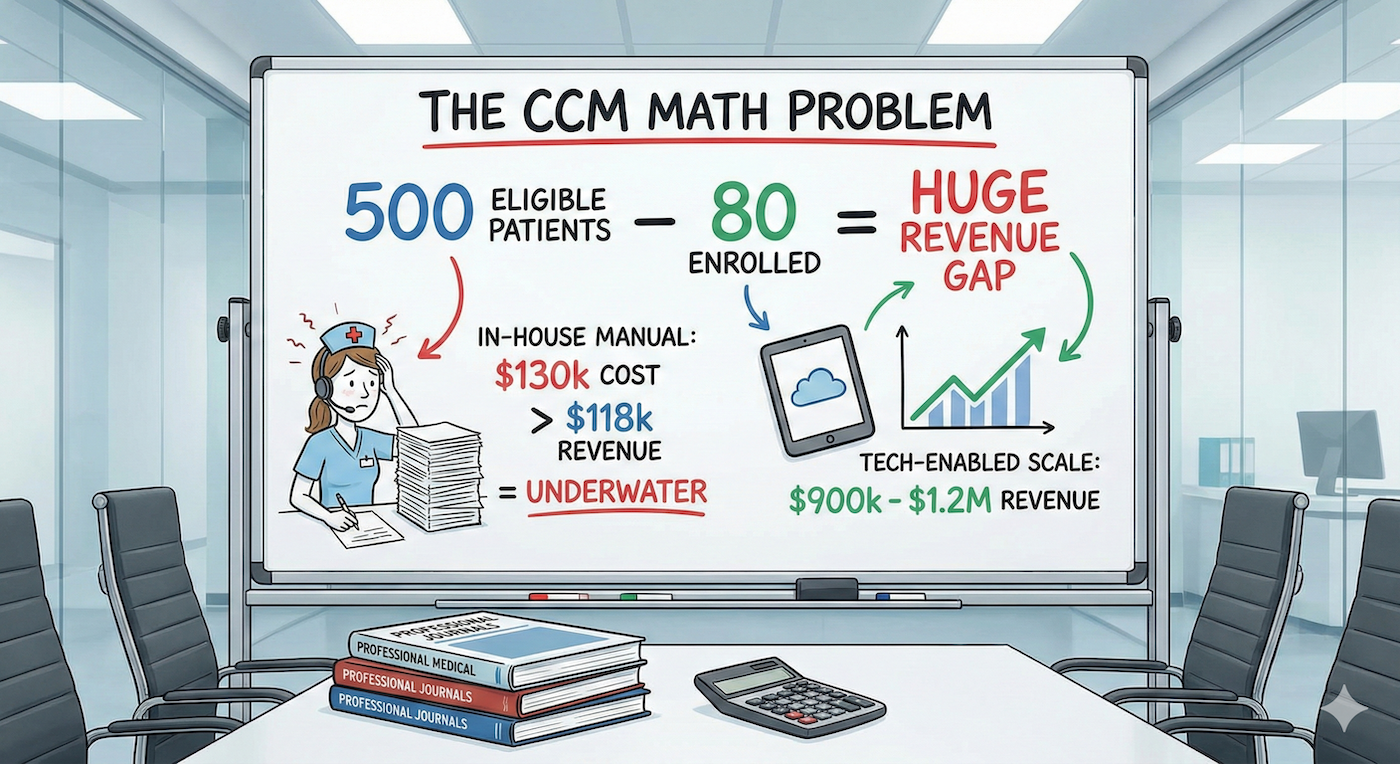
I ask how many patients are enrolled. The answer is usually somewhere between 40 and 100. I ask how many Medicare patients in their panel have two or more chronic conditions. They pause. The answer, once they look it up, is almost always north of 500.
That gap between 80 enrolled and 500 eligible isn't a staffing problem. It's a math problem that most practices have never actually worked through.
Let's be specific. In 2026, a Chronic Care Management nurse costs approximately $90,000 to $100,000 per year in salary alone. Once you factor in benefits, payroll taxes, PTO, malpractice coverage, and management overhead, the fully loaded cost lands closer to $120,000 to $140,000 annually.
That nurse needs to spend a minimum of 20 minutes per patient per month to bill the base CCM code (99490), which reimburses approximately $66 under the 2026 Medicare Physician Fee Schedule. But 20 minutes of patient-facing time doesn't account for documentation, care plan updates, coordination calls with specialists, follow-up scheduling, and the administrative work that surrounds every clinical touchpoint.
In reality, when you account for all the non-billable time, a single nurse running CCM manually can effectively manage somewhere between 80 and 150 patients. That's the ceiling before quality starts to degrade, documentation gets sloppy, and patients start falling through the cracks.
So here's the math. Take the optimistic end: 150 patients at $66 per month in base CCM reimbursement. That's $118,800 per year in gross revenue. Against a fully loaded nurse cost of $130,000, you're underwater before you've paid for a single piece of technology, a phone system, or a supervisor's time.
This is why most internal CCM programs stall at 50 to 80 patients. The practice leader looks at the P&L, sees a break-even or money-losing line item, and concludes that CCM doesn't pencil out. The program doesn't get killed. It just never gets funded to grow.
The problem with that conclusion is that it's based on a fraction of the available revenue. Most internal programs are billing 99490 and stopping there.
The 2026 fee schedule tells a different story when you look at the full code set. The add-on code for an additional 20 minutes of clinical staff time (99439) reimburses approximately $50 per month. Complex CCM (99487) for patients requiring moderate to high complexity medical decision-making pays roughly $144 for the first 60 minutes. Layer in RPM codes for patients who also qualify for remote physiologic monitoring, and you're looking at combined per-patient-per-month revenue that can reach $150 to $250 depending on the patient's condition profile and the services delivered.
CMS increased CCM reimbursement by roughly 10% for 2026, the largest bump the program has seen. RPM saw an even bigger effective increase, around 25%, driven by new codes that lower the data submission threshold from 16 days to just 2 days per month. That change alone makes approximately 20% more patients eligible for RPM billing than were eligible last year.
The revenue opportunity for a practice with 500 eligible patients isn't $400,000. It's closer to $900,000 to $1.2 million annually when the full code set is utilized effectively, patients are stratified by acuity, and RPM is layered on top of CCM for qualifying patients. But capturing that revenue requires a staffing model and technology infrastructure that most private practices simply aren't set up to support.
The instinct is to throw headcount at the problem. If one nurse can handle 150 patients, hire three or four and scale to 500. On paper, it works. In practice, it creates a different set of problems.
First, there's the hiring timeline. The nursing labor market remains tight, and experienced RNs with care management skills aren't sitting on the bench waiting for your job posting. Recruiting, credentialing, and onboarding a single CCM nurse takes 60 to 90 days in a good market. Scaling a team of three or four takes the better part of a year.
Second, there's the management burden. Someone in the practice has to supervise the CCM team, manage quality, ensure compliance with CMS documentation requirements, handle scheduling, and deal with turnover. That's either a new role you're creating or existing bandwidth you're pulling from somewhere else.
Third, and this is the one most practices don't think about until it's too late: the billing complexity scales faster than the clinical work. Every patient-month requires accurate time tracking, proper code selection, documentation that meets CMS audit standards, and coordination with your billing team to ensure claims go out correctly. One compliance mistake across a 500-patient panel can trigger an audit that costs more than the entire program generated.
The result is predictable. The practice hires one nurse, runs 80 patients, decides it's not worth the headcount investment, and leaves 400+ eligible patients unmanaged. Those patients continue to cycle through ER visits, hospital admissions, and specialist referrals that the practice never captures downstream revenue from.
The practices that scale CCM successfully don't do it by adding nurses linearly. They change the ratio of patients per care manager by using technology to eliminate the manual work that eats clinical time.
This is where AI and automation become relevant in a way that actually matters, not as a buzzword, but as the thing that turns a 1:150 nurse-to-patient ratio into something closer to 1:300 or 1:400. When care coordination software handles outreach scheduling, automates documentation, flags rising-risk patients before they decompensate, and routes clinical decisions to the right level of the care team, nurses spend their time on actual clinical work instead of administrative overhead.
The difference is structural. At a 1:150 ratio, your economics are marginal at best. At 1:300, you're operating a program that generates meaningful margin while delivering measurably better care. The nurse isn't working harder. She's working on the patients who need her most while technology handles the rest.
This isn't theoretical. Programs built on this model routinely achieve 40%+ profit margins on CCM revenue while maintaining clinical quality metrics that exceed what most internal programs produce at a fraction of the scale.
The question isn't whether CCM works. CMS wouldn't have increased reimbursement 10% in a single year if the program wasn't producing results. The question is whether your current approach to CCM can scale to the size of the opportunity sitting in your patient panel.
If you're running 80 patients internally and calling it a program, you're leaving somewhere between $500,000 and $1 million in annual revenue on the table. More importantly, you have hundreds of patients with multiple chronic conditions who aren't getting the coordinated care between visits that prevents the hospitalizations and ER visits that drive up cost for everyone.
The math doesn't lie. The practices that figure out the staffing model and technology infrastructure to operate CCM at scale will outperform the ones that treat it as a side project. With the 2026 fee schedule increases, the gap between those two groups is only going to widen.
The economics have never been more favorable. The question is whether you're set up to capture them.
