
CMS just handed provider organizations the most meaningful expansion of remote care reimbursement in a decade, and most leadership teams are reading it like a CPT code memo. That is a mistake. The January 1, 2026 Physician Fee Schedule changes, combined with a nursing workforce that has lost more than 138,000 clinicians since 2022 and a value-based care transition that C-suites say they will accelerate over the next 24 months, represent a structural shift in how chronic disease gets managed and paid for in this country.
The organizations that understand this are already redesigning their care models. The ones that do not will watch their margins compress while competitors build recurring, high-margin revenue lines on top of patient populations they already own.
Under the 2026 Final Rule, CMS introduced two new Remote Patient Monitoring CPT codes (99445 and 99470) that allow billing for as few as 2 to 15 days of data transmission per 30-day period, and for management time as short as 10 minutes. For years, the 16-day and 20-minute floors were the silent gatekeepers that kept RPM locked to the sickest, most adherent patients. That gate is now open. Shorter care episodes, post-discharge windows, medication titration periods, and behavioral health check-ins all become reimbursable activities. CMS also increased reimbursement on existing CCM codes by roughly 10 percent and finalized the mandatory Ambulatory Specialty Model for heart failure and low back pain, which puts specialists on the hook for outcomes in two of Medicare's highest-cost categories.
Translation for a CFO: the addressable patient population for remote care just expanded by an order of magnitude, and the per-patient economics got better.
Translation for a CMO: the clinical thesis that remote care belongs only with the top five percent of chronic patients is now a compliance thesis, not a care thesis.
Here is what nobody wants to say out loud. You cannot staff the expanded opportunity. More than 138,000 nurses left the workforce between 2022 and 2024, and 40 percent of remaining nurses report intent to leave or retire within five years, according to AHA reporting. The labor market will not bail out a care model that requires adding human hours in linear proportion to expanded billing eligibility.
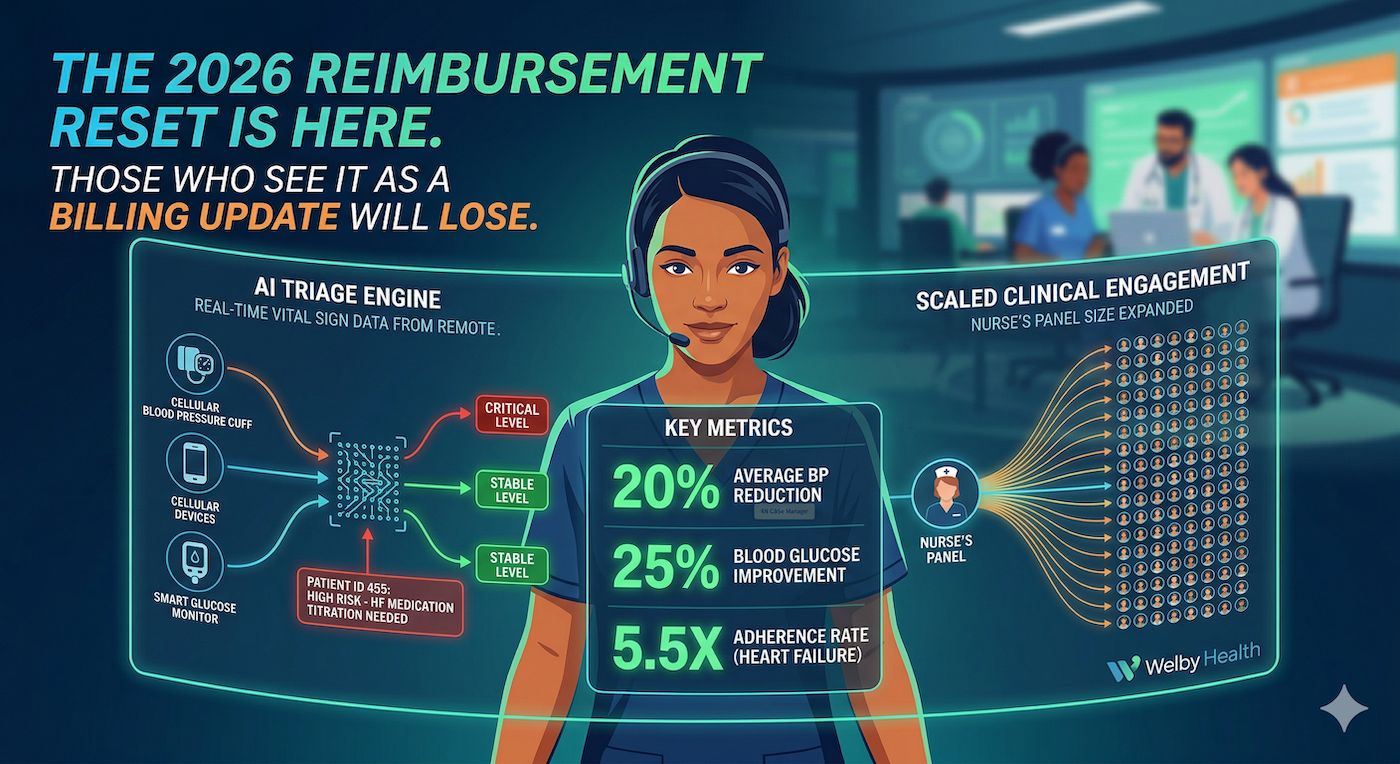
The only way the 2026 reimbursement expansion translates into actual clinical and financial outcomes is if clinicians operate at the top of their license while software handles the rest. That means automated vital sign monitoring, AI-driven triage that tells the nurse which of 400 patients needs attention in the next hour, medication adherence tracking that does not rely on self-report, and patient communication that is personalized at scale without burning out the people running it.
This is not a distant vision. Healthcare IT News reported this quarter that 2026 is the year AI stops being a reporting layer in RPM and becomes the active triage and personalization engine. The organizations already operating this way are seeing outcomes that frankly should embarrass the status quo.
When licensed RN case managers are paired with AI-powered workflows, the outcomes stop looking like incremental improvement and start looking like a different category of medicine. At Welby, we see a 20 percent reduction in blood pressure among patients using cellular-enabled BP cuffs, a 20 percent or greater reduction in blood glucose within four weeks for patients on smart glucose monitors, and heart failure patients who are 5.5 times more likely to adhere to the life-saving therapies their physicians prescribed. Those are not marketing numbers. They are what happens when you remove the friction between the patient's living room and the care team's queue.
The model works because the software does the watching and the humans do the caring. Automated vital sign capture, algorithmic risk stratification, and intelligent communication routing mean a single nurse can meaningfully engage with a panel size that would have been malpractice five years ago. Patients get more attention, not less, because the attention is targeted at the right moments instead of spread thin across everyone on a Tuesday.
If you run a health system, a specialty group, a primary care network, or an ACO, you have three choices heading into the back half of 2026.
One, treat the CMS changes as a coding update, pass them to your revenue cycle team, and hope the pilot you launched in 2023 can absorb the expanded scope. This is the path of quiet margin erosion.
Two, build the capability internally. Hire the nurses you cannot find, build the software you do not specialize in, and absorb the 18 to 24 months of operating losses while you figure out what your competitors already know.
Three, partner with a platform built for exactly this moment. Get the clinical staffing, the AI-powered workflows, the device logistics, and the billing infrastructure as a single integrated service, and turn a previously unreimbursed operational burden into a new revenue line that generates billable activity under CCM, RPM, and TCM codes while improving the outcomes your value-based contracts are measured against.
The math on the third option is the reason 76 percent of health system C-suites told Fierce Healthcare they plan to increase value-based care participation in the next two years. They have seen the spreadsheet. They know the specialty model for heart failure is mandatory, not optional. They know the workforce is not coming back in its old form.
Reimbursement policy does not often create an inflection point. When it does, the leaders who move first compound the advantage for a decade. The 2026 rule is that kind of moment. The organizations that build a remote care engine now, whether internally or through the right partner, will own the chronic patient relationship, the downstream procedural volume, and the value-based contract performance that defines the next era of healthcare economics.
The ones that wait will spend 2027 trying to catch up to competitors who stopped treating chronic care as a cost center and started treating it as the front door.
The policy environment finally caught up with what the technology has been ready to do for three years. The only question left is whether your organization moves before the window closes.
CMS's 2026 Final Rule lowered the RPM threshold from 16 days and 20 minutes to as few as 2 days and 10 minutes, raised CCM reimbursement roughly 10 percent, and made the Ambulatory Specialty Model for heart failure and low back pain mandatory. Combined with a nursing workforce that has lost 138,000+ clinicians since 2022, the expansion only works if clinical teams are paired with AI-driven triage, automation, and communication. Health systems that treat this as a billing update will see margins erode while competitors build recurring revenue lines on top of their existing chronic patient populations. The winning move is to turn chronic care into the front door of the organization, not a cost center behind it. The window to move first is open now and will not stay open long.