The application window for the first cohort of CMS's ACCESS model closed on April 1. If you submitted, you already know what is coming. If you did not, you need to understand what this model signals for every provider organization managing chronic disease in Medicare.
ACCESS, which stands for Advancing Chronic Care with Effective, Scalable Solutions, is a voluntary 10-year payment model launching July 5, 2026. It introduces something CMS is calling Outcome-Aligned Payments. The concept is straightforward: participating organizations receive recurring payments for managing patients with qualifying chronic conditions, but they only earn the full amount when patients hit measurable health outcomes.
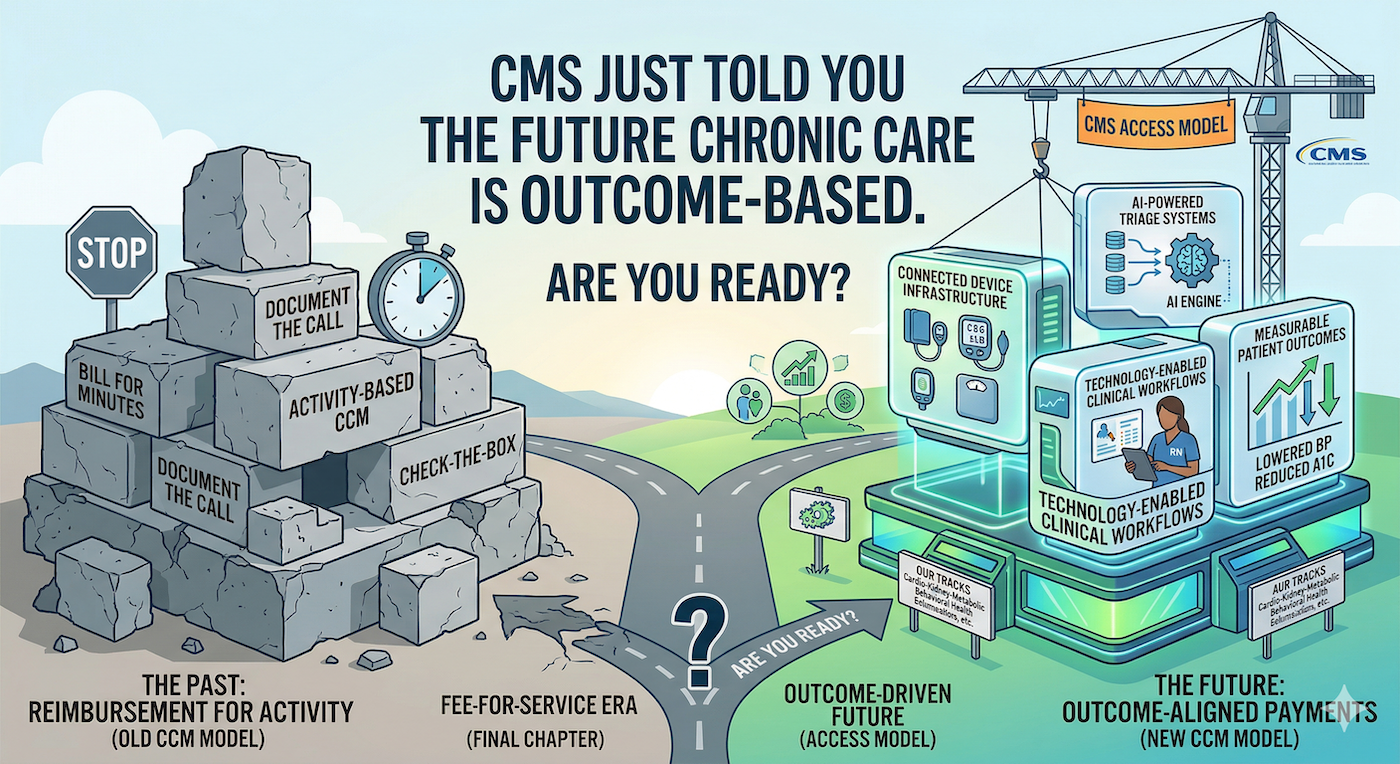
This is not a pilot buried in a regulatory footnote. This is CMS telling the market, in plain language, that the fee-for-service era for chronic care management is entering its final chapter.
For years, chronic care management reimbursement has been activity-based. Bill for 20 minutes of non-face-to-face care coordination. Document the phone call. Check the box. The payment arrives regardless of whether the patient's blood pressure improved, their A1C dropped, or they avoided the emergency department.
ACCESS flips that model. It focuses initially on four clinical tracks covering conditions that affect roughly two-thirds of Medicare beneficiaries: an Early Cardio-Kidney-Metabolic track (hypertension, dyslipidemia, obesity, prediabetes), a Cardio-Kidney-Metabolic track (diabetes, chronic kidney disease, atherosclerotic cardiovascular disease), a Musculoskeletal track (chronic pain), and a Behavioral Health track (depression and anxiety).
Participating organizations must be Medicare Part B-enrolled providers or suppliers, designate a physician clinical director, and comply with HIPAA and applicable FDA requirements. CMS is also building an ACCESS Tools Directory to help participants identify software, connected clinical devices, and interoperability solutions that support model compliance.
The message to health system leaders: this is not just a reimbursement change. It is an infrastructure requirement. You cannot manage outcomes at scale without the technology and clinical workflows to actually move the needle on patient health.
The timing of ACCESS matters. It arrives alongside several other signals that the market is shifting decisively toward value and outcomes.
Starting January 1, 2026, CMS loosened RPM and RTM billing requirements, reducing minimum patient data collection days from 16 to as few as 2 and lowering the management time threshold to 10 minutes. These are among the most significant changes to remote monitoring reimbursement in years. The intent is clear: CMS wants more patients monitored, more data flowing, and more interventions happening between office visits.
Meanwhile, value-based care arrangements are projected to cover 45% of Medicare beneficiaries by the end of 2026. AI adoption among U.S. healthcare providers has reportedly jumped from 34% in 2024 to a projected 68% this year. And the healthcare workforce gap continues to widen, with projections showing a 12% shortfall between clinical staffing needs and available practitioners.
Put these pieces together and the picture is not subtle. The system is moving toward a model where technology-enabled, outcome-driven chronic care is not optional. It is the baseline expectation. Provider organizations that are still running chronic care management as a manual, labor-intensive, check-the-box operation are building on a foundation that CMS is actively moving away from.
Here is the question every health system CEO and CFO should be asking right now: if CMS called tomorrow and said your chronic care management payments depend on whether your hypertensive patients actually lowered their blood pressure, could your current infrastructure deliver?
For most organizations, the honest answer is no. Traditional CCM programs are built around phone calls, manual documentation, and retrospective chart reviews. They generate billing activity but they are not designed to drive and measure clinical outcomes in real time.
The organizations that will thrive under outcome-aligned models are the ones investing now in three capabilities. First, connected device infrastructure that gives clinical teams continuous visibility into patient vitals between visits, not just snapshots during quarterly appointments. Second, AI-powered triage systems that can identify rising-risk patients before they decompensate, flagging concerning trends so care teams can intervene proactively rather than reactively. Third, licensed clinical staff embedded in technology-enabled workflows, not replacing nurses with algorithms but giving nurses the tools and intelligence to manage larger panels without sacrificing quality.
This is the model we have built at Welby Health. Our platform pairs licensed RN case managers with our MARKUS AI engine, which continuously monitors patient data from cellular-enabled blood pressure cuffs, smart glucose monitors, and weight scales. When MARKUS identifies a concerning trend, the nurse is notified instantly and can act, whether that means counseling a patient on medication adherence, adjusting a care plan, or escalating to a physician. The results reflect what outcome-aligned care looks like in practice: 20% decreases in blood pressure, 20%-plus reductions in blood glucose within four weeks, and heart failure patients who are 5.5 times more likely to adhere to life-saving therapies.
These are not theoretical projections. They are the kinds of outcomes that CMS is now building payment models around.
ACCESS is a 10-year model. Applications for the January 2027 cohort are still ahead. But the strategic implications are already here.
If your organization treats chronic care management as a compliance exercise, the reimbursement landscape is about to leave you behind. If you treat it as a clinical and financial strategy, powered by connected devices, AI-driven workflows, and skilled clinical teams, you are positioned for what comes next.
The shift from activity-based to outcome-based payment is not a trend. It is a policy direction backed by a decade-long CMS commitment. The organizations that recognized this early and invested in the technology and clinical infrastructure to deliver measurable outcomes will be the ones that capture the value.
The rest will be playing catch-up in a market that has already moved on.
TL;DR: CMS's new ACCESS model, launching July 5, 2026, introduces outcome-aligned payments for technology-enabled chronic care management across conditions like hypertension, diabetes, chronic pain, and depression. This is a 10-year model that ties full reimbursement to measurable patient health outcomes, not just documented activities. Alongside loosened RPM billing rules and accelerating value-based care adoption, the signal to health systems is clear: chronic care management programs that cannot demonstrate real clinical outcomes are on borrowed time. Provider organizations need connected device infrastructure, AI-powered clinical triage, and technology-enabled nursing workflows to compete in what comes next.
