
CMS just made its strongest pro chronic care move in five years. UnitedHealthcare, the largest commercial payer in the United States, tried to walk away from remote patient monitoring for most chronic disease in the same window. They postponed it under industry pressure. They did not kill it.
If you run a health system, a multispecialty group, or a primary care network, this is not a quiet quarter for chronic care strategy. The reimbursement map is splitting in real time, and the operating model you choose between now and the 2027 fee schedule cycle will determine whether your chronic care program is a margin engine or a cost center.
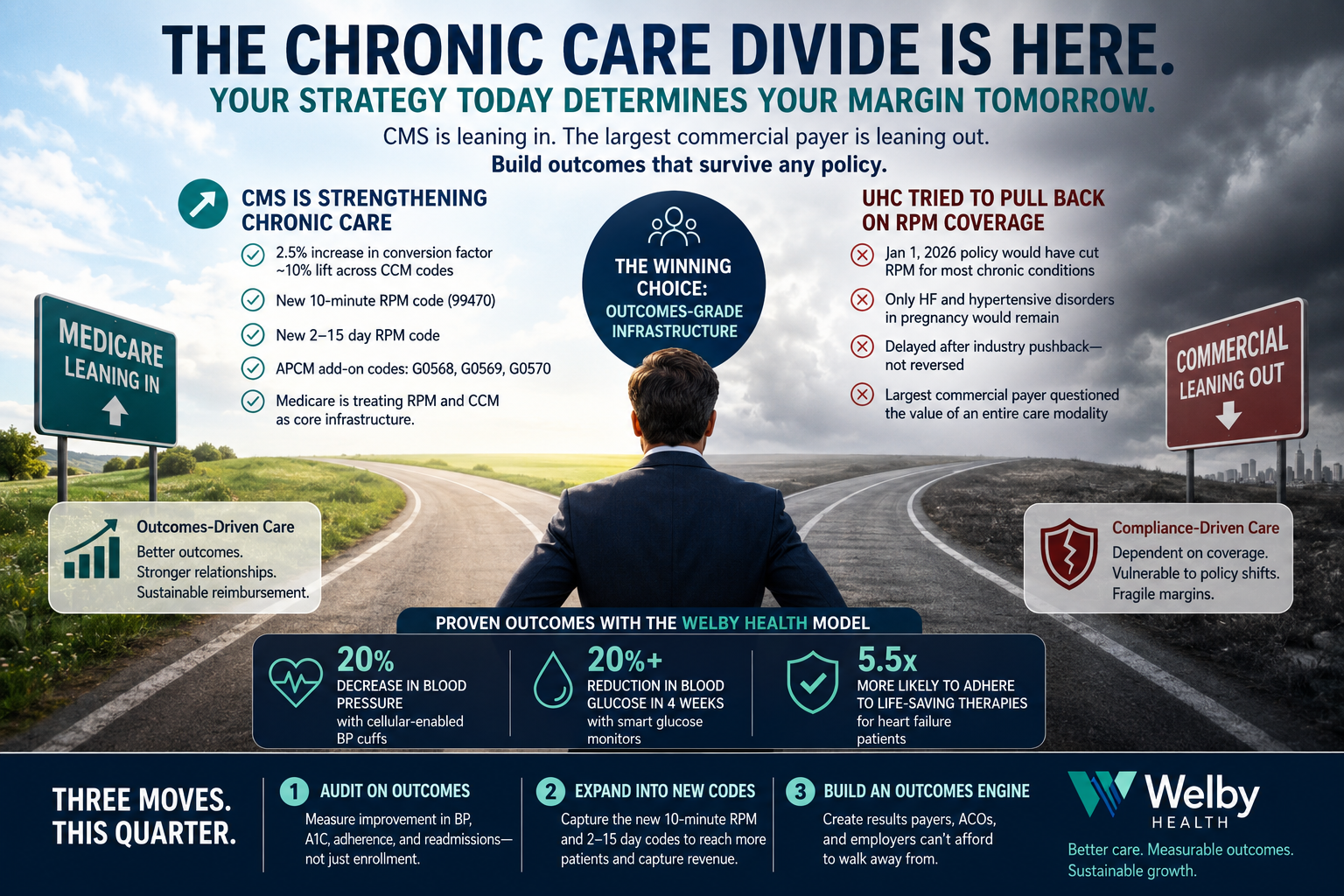
For the first time in five years, CMS finalized an increase in the Medicare physician fee schedule conversion factor, with a 2.5 percent increase in the payment rate, translating to roughly a 10 percent lift across chronic care management codes. That is not a rounding error. For practices managing thousands of CCM patients, it is meaningful new revenue with zero additional clinical effort.
More importantly, the 2026 rule expanded the RPM framework in ways that change who is reachable. CMS added CPT 99470, a new 10 minute RPM care management code that finally lets clinicians bill for shorter, targeted interventions. They added a code for two to 15 days of measurements, breaking the old 16 day data floor that excluded large patient populations from reimbursement entirely. Patients who transmit data inconsistently, patients in acute medication adjustment, and patients in the first weeks of monitoring are now fully eligible.
CMS also finalized the new APCM add on codes, G0568, G0569, and G0570, which mirror existing BHI and CoCM codes and create a parallel revenue pathway for advanced primary care management layered with behavioral health integration.
Read the policy plainly. Medicare is treating remote monitoring and chronic care management as core infrastructure for the Medicare population. Not as an experiment. Not as a nice to have. As infrastructure.
In the same months CMS was strengthening RPM, UnitedHealthcare announced a January 1, 2026 policy that would have eliminated RPM coverage for most chronic conditions across its Medicare Advantage, Community Plan, and commercial books. Under the announced policy, only patients with heart failure or hypertensive disorders during pregnancy would have remained covered. General hypertension, Type 2 diabetes, and COPD would have lost RPM coverage entirely.
UHC's stated justification, that there is no evidence supporting RPM's value for these conditions, runs against the weight of peer reviewed literature showing reduced emergency visits, improved medication adherence, and better outcomes. After fierce industry pushback, on December 17, 2025, UnitedHealthcare delayed implementation. The delay is not a reversal. It is a postponement. The underlying restrictions can resurface in any future policy cycle, and the largest commercial payer in the country has now publicly questioned the value of an entire care modality.
That should land hard for anyone running a chronic care P and L.
We are out of the era when chronic care infrastructure could be built to one payer's spec. The reimbursement environment is now bifurcated. Medicare is leaning in. The largest commercial payer is leaning out. Other commercial payers will pick a side, and they will not all pick the same one.
There are two paths in front of provider executives right now.
Path one is to build to the lowest common denominator. Cover only the conditions and modalities every payer reimburses today, accept that your chronic care program is essentially Medicare only, and treat the commercial population as a billing exception. This path is operationally simple and strategically fragile. The day a major payer cuts a code, your model breaks.
Path two is to build a chronic care operation whose clinical results are strong enough that reimbursement debates become secondary. If your program demonstrably reduces emergency visits, reduces readmissions, improves adherence, and lowers total cost of care, you stop being a vendor that depends on a payer's coverage policy. You become a partner that payers, employers, ACOs, and at risk providers actually want to keep paying, regardless of which CPT code is in or out this year.
This is the divide. Outcomes grade chronic care infrastructure survives any payer policy environment. Compliance grade chronic care infrastructure dies the moment a single payer changes its mind.
The teams that come out ahead in this divergence are not the ones running the largest enrollment numbers. They are the ones whose clinical results are strong enough to be defensible in front of any payer medical director, any value based contract negotiator, and any patient who has the choice to leave.
At Welby Health, we have built our operating model around that thesis. Our chronic care platform pairs licensed RN case managers with AI powered workflows that automate vital sign monitoring, medication adherence tracking, and patient communication. The point of the AI layer is not to replace clinicians. It is to make every clinician carry a larger panel without sacrificing the human relationship that drives adherence.
The outcomes follow. Patients in our program have seen a 20 percent decrease in blood pressure with cellular enabled BP cuffs. We have measured a 20 percent or greater reduction in blood glucose in four weeks with smart glucose monitors. Heart failure patients in our program are 5.5 times more likely to adhere to life saving therapies. Those are the numbers that hold up in any reimbursement environment.
That same model also captures the full revenue stack the 2026 rules open up. CCM. RPM, including the new 10 minute code and the 2 to 15 day code. TCM for post discharge transitions where readmission risk and revenue capture both live. APCM add ons where behavioral health integration applies. The codes change. The clinical engine does not.
Three moves, in order.
First, audit your current chronic care vendor or in house program on outcomes, not enrollment. If your dashboard shows enrolled patients but cannot show measurable improvement in BP, A1C, adherence, or readmissions, you are exposed.
Second, expand into the new codes that just opened up. The 10 minute RPM code and the 2 to 15 day code are not minor. They are how you reach the patients your current 20 minute and 16 day thresholds exclude, including the highest risk patients in the early weeks of a new diagnosis or medication change.
Third, decide what you actually want from your chronic care program. If the goal is incremental Medicare revenue, the 2026 rule gives you a tailwind. If the goal is to be the operator that payers, ACOs, and employers cannot afford to drop, build the outcomes engine now, while the divergence is still visible and your competitors are still arguing about coverage policy.
The next three years will not be friendly to providers who treat chronic care as a billing motion. They will be very friendly to providers who treat it as a clinical product with measurable results.
Pick the side of the map you want to be on. The window to choose is shorter than it looks.
Seth Merritt is the Founder and CEO of Welby Health, where licensed RN case managers and AI powered workflows deliver chronic care management, remote patient monitoring, and transitional care management for health systems, provider groups, and at risk organizations.